Mistake Proofing with Choice Architecture
Engineering Systems and Software For Quality
In Thaler and Sunstein's book, Nudge, we discover that decision choices can be engineered to optimize the response. When you purchase something on a website, there's a checkbox for receiving ongoing promotions. If the box is not checked, you have to opt in; if the box is checked, however, you have to opt out. As a salesperson, you want the box checked because that's the response you want.
There's No Such Thing as a Neutral Choice Architecture
While I hate having to opt out of every SPAM opportunity, I understand why it's there. It should be obvious that there's no such thing as a neutral choice architecture. Every machine, every procedure, every document and every software system has a choice architecture built into it. The only question is: "Is it a useful choice architecture or does it encourage mistakes and errors?"
Mistake Proofing with Choice Architecture for Health Care
Here's an example from http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3818966/: "It has been demonstrated that changing the default settings on
ventilators to ‘provide lower air volumes into patient's lungs' led to a
25% decrease in mortality.83 When the default setting was changed, this took advantage of the fact that the intensive care physicians (like all of us) exhibit a bias for the status quo."
Designing Choice Architecture into Software Systems
I spent over 20 years developing software for mainframe, mini and micro computers. Crunching the numbers was easy. Adding, changing and deleting data was easy. The human interface was always the trickiest part.
Recently, I was working with a healthcare system. It was having trouble getting physicians to document a patient's risk for blood clots (VTEs) and physicians were sometimes prescribing chemical and mechanical prophylaxis unnecessarily. The physician was doing the risk assessment in their head, but not noting it in the medical record. Here's my simple suggestion for how to mistake-proof handling VTEs:
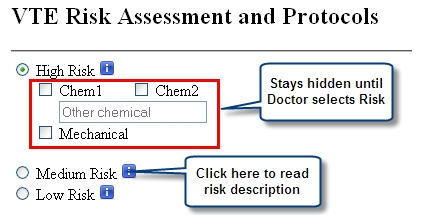
By making the risk assessment the first step in prescribing prophylaxis, doctors would record the risk assessment first, then get chemical (e.g., blood thinners) and mechanical options for prevention. Low risk patients do not need mechanical prophylaxis, so that option could be eliminated.
Default options can be strong nudges. Evidence-based medicine would suggest that some of these options are better than others and could be pre-checked. What if one chemical was safer than another? Could it be the default choice? What if one option was contraindicated for a certain level of risk? Could it be eliminated from the menu?
Similarly, at Virginia Mason's Back Pain clinic, doctors cannot order MRIs for "uncomplicated" back pain. This cut unnecessary and expensive MRIs dramatically. And it freed up the MRI for more important work.
Highlight the Positive
Studies have shown that describing the positive will increase that choice. Why do you think TV ads say that 90 percent of dentists recommend brand toothpaste? Why do doctors say "90 percent of patients survive this surgery rather than 10 percent die?" The positive influences the choice made.
Here's my point:
Humans are lazy. They will follow the path of least resistance. We can design systems and procedures to leverage our natural instincts or we can let existing systems that were often designed without thought dictate the results. Isn't it time to mistake-proof these decisions?
Need help designing a choice architecture for your software application? Consider using Jay's experience to help you optimize your results.
Rights to reprint this article in company periodicals is freely given with the inclusion of the following tag line: "© 2015 Jay Arthur, the KnowWare® Man, (888) 468-1537, support@qimacros.com."
Hire Jay Arthur to train your staff in his one-day Lean Six Sigma Workshop! Contact Jay at 1-888-468-1537.
Join 100,000+ Users
in 80 Countries